Dr. Levy's CBT Blog
Insights on Well-Being, Contentment, and Cognitive Behavioral Therapy
|
Let's say you have an important work deadline coming up, or an important meeting, or a job interview. You'll likely be a bit stressed about it, right? That's understandable - and useful! A reasonable amount of stress shows that we care about these critical tasks and can actually help us prepare better for them. However, every now and then, that stress gets out of hand...instead of encouraging us to be ready for the challenge, the stress mounts so high that it makes that challenge seem completely unattainable. In the early 1900s, psychology researchers Robert Yerkes and John Dodson developed an empirical curve that illustrates our performance levels on a task relative to the stress levels present in that situation. It is easy to understand if you think about it in terms of a test at school. If there is no stress at all, we won't really prepare for the test, and might show up on the exam day without having done any studying. A good amount of worry and stress will encourage us to prepare for the test by reading the book chapters and doing the practice exercises, once...or maybe twice. An amount of stress beyond that might lead us to re-read all those chapters and re-do the practice exercises a few too many times, to the point where we may be too tired by the time the test comes along to get the best grades. And if we are really, really scared of the test, telling ourselves that it's way too difficult and we will never get a good grade on it, we may just throw our hands up in the air and not study for it at all. We may give up before we start, out of panic, exhaustion, and fear. So, some stress is good. Too little or too much may lead to subpar performance. The question is how to modulate the stress to get it to the level that is good for you. There are many answers there, ranging from relaxation exercises to worry break and mindfulness moments to reappraising the importance and threat of the situations ahead. In TEAM-CBT, we have some great tools that can help with all of those! 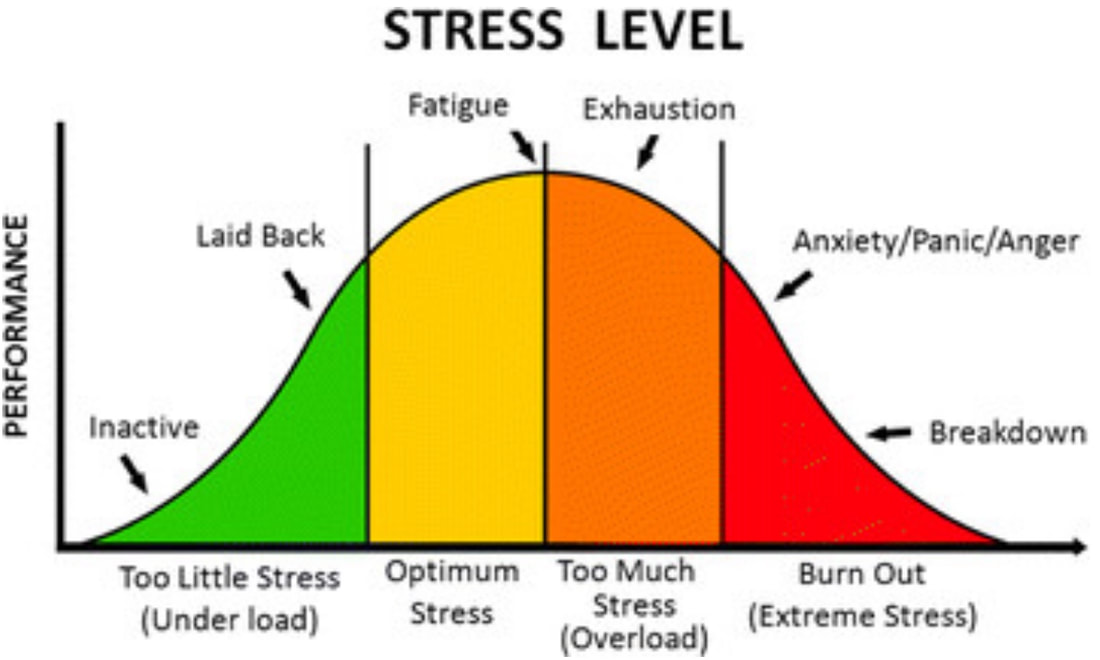
0 Comments
A client recently shared with me a video of actor Will Smith talking about the fear that he felt before he was scheduled to go on a skydiving trip. That prompted a discussion around the difference between fear and anxiety. To my way of thinking, fear is to anxiety as concrete is to imagined, actual is to forecast, or today is to tomorrow. From a cognitive standpoint, fear pertains to a real, tangible, identifiable, and often immediate source of danger. For example, if a lion is standing in front of me, I will be afraid (not anxious!). If I am about to jump out of a plane, standing by the open door at 3,000 feet, I will be afraid (not anxious!). On the other hand, anxiety applies to situations where I perceive a potential for danger. I have not yet seen the lion, but I think that the lion may be lurking close by. Or coming for me at any time. Or just feeling hungry. I worry about something that has not happened yet and may never happen, But then, it could conceivably happen. In psychotherapy, we may address both fears and anxiety using Cognitive Behavior Therapy. Problematic fears often come up in the context of phobias (e.g., fear of flying or driving across bridges). Clinically-relevant anxiety tends to manifest itself in the form of excessive worrying, tension, restlessness, over-sensitivity and hypervigilance. Both feelings trigger our "fight or flight" response mechanism, which I will describe in more details in my next blog post. The treatment of choice most often involves Exposure Therapy, an evidence-based intervention in which the client learns how to gradually expose themselves to stimuli that they fear, with a lot of support and guidance from the therapist. In the meantime, here is Will Smith talking about his "fears," which actually pertain to both anxiety and fear. Enjoy! Before starting therapy, clients often wonder "How long will I be in therapy?" This funny video from The Onion provides a clever satire of the open-ended, long-term model of therapy that is often portrayed by the popular media: Cognitive behavioral therapy (CBT) tends to operate within a much more short-term, focused model of psychological intervention that aims to reduce current symptoms, address specific problems, and build skills that the client can take with him/her after treatment ends. Hence, treatment length is usually measured in weeks or months, rather than years or decades.
Indeed, there is ample research evidence that response to psychotherapy follows a 'negatively accelerated' curve where more and more effort is required to achieve smaller and smaller changes (that is called a log-normal curve for the math geeks out there). Dr. Ken Howard was the first to analyze this correlation and posit markers for response to psychotherapy according to dosage. Here is his original article. The original dose-effect study was run in 1986, based on psychodynamic or interpersonal treatment only, with the following findings: * About 15% of patients improve before the first session of therapy * 50% of patients typically improve at 8 sessions * 75% of patients typically improve at 26 sessions * 85% of patients typically improve at 52 sessions It is possible that modern psychological techniques have accelerated that theoretical curve in the past 30 years. In practice, however, there are many factors influencing the right dose of psychotherapy for each client, including diagnosis, acuity, readiness to change, social circumstances, and frequency of treatment (more regular treatment is shown to be more effective). But what we can glean from the data above is that longer and longer treatment periods may indeed offer diminishing gains at increasing levels of effort. With CBT, you and your therapist will have powerful tools for change readily available. The specific length of psychotherapy treatment will vary for each person and each presenting problem. But with commitment and focus in the context of a true partnership, CBT can lead to fast and meaningful change. Empathy is a fundamental ingredient of any psychotherapy treatment. It is so important in TEAM-CBT that it gets its own letter in the acronym: The 'E' in TEAM actually refers to the phase of treatment when offering and receiving empathy is the main goal. In my experience, it is a necessary - although most often not sufficient - element for successful therapy. Through empathy, the therapist attempts to develop a deeper understanding of the client's idiosyncratic experiences in certain situations. That hinges on the therapist's ability to put themselves in the place of the client, reflecting the client's thought processes and feelings, acknowledging the client's strengths and struggles, and sharing, in a professional manner, the impact that these aspects have had on them, the therapist. With clear communication and a genuine desire to connect, empathy builds a sense of shared experience that allows the therapeutic alliance to flourish. Empathy is not sympathy, though. Empathy is a process where two people meet at the same level. In sympathy, one 'stronger' player attempts to rescue the 'weaker' one, often times by minimizing their experience in a well-meaning maneuver to quickly sweep away negative feelings. Renowned researcher Dr. Brene Brown has developed a short video that illustrates this distinction. It's well worth three minutes of your time: As we go through our busy days, we are asked to form spur-of-the-moment opinions about the events around us. Someone says hi? [They want something from me!] Someone fails to say hi? [I have done something to offend them!] Car doesn't start? [This always happens to me!] Late for work? [The world is conspiring against me!]. We all have these scripts inside our heads that help us evaluate things that happen in our lives quickly and efficiently. Unfortunately, not always accurately.
In the process of coming up with these quick appraisals of events happening in our lives, we often take 'shortcuts' that we hope make the evaluation process quicker. It might. But the shortcuts often take us in directions that are not helpful. In cognitive psychology, we have grouped these unhelpful shortcuts in categories with labels that describe each one of them. They are called Cognitive Distortions. Dr. David Burns describes them as follows: 1. All-or-nothing thinking (also known as 'black and white thinking'): You look at things in absolute, black-and-white categories, e.g. "I never do anything right!" (seriously, never ever??) 2. Overgeneralization: You view a negative event as a never-ending pattern of defeat, e.g. "I can't make anyone happy" (when you have a fight with your boyfriend, without remembering how much you mean to your best friend!) 3. Mental filter: You dwell on the negatives and ignore the positives, e.g. "I am really bad at sports" (you lose a soccer game, and forget how good you are at indoor cycling). 4. Discounting the positives: You insist that your accomplishments or positive qualities don’t count, e.g. "My good grade in this test was a stroke of luck" (after studying two days for it!). 5. Jumping to conclusions: You jump to conclusions not warranted by facts. These include mind-reading (assuming that people are reacting negatively to you) and fortune-telling (predicting that things will turn out badly), e.g. "She doesn't like me" or "I know I will not get this job." 6. Magnification or minimization: You blow things way out of proportion or you shrink their importance, e.g., "This is the only important interview I will ever have." 7. Emotional reasoning: You reason from how you feel: “I feel like an idiot, so I must be one.” 8. “Should” statements: You criticize yourself or other people with “shoulds,” “shouldn’ts,” “musts,” “oughts,” and “have-tos,” e.g., "my life should be way more exciting!" 9. Labeling: You give yourself a label on the forehead. E.g., instead of saying, “I made a mistake,” you tell yourself, “I’m a jerk” or “I’m a loser.” 10. Blame: You blame yourself for something you weren’t entirely responsible for, or you blame other people and overlook ways that you contributed to a problem, e.g., "I am a bad teacher" (when you forget how difficult your students are...) or "They are bad students" (when you fail to analyze your teaching skills beforehand). We all make these thinking errors on a daily basis. At times, they can go unnoticed. More often, they will lead to feelings of sadness, anger, hopelessness, anxiety and more. The good news is that, with practice, it is easy to identify these distortions and learn how to fix them. Cognitive therapy is just the answer if you are looking to lear more about your thought patterns and how to change them. "Impostor syndrome" (also known as impostor phenomenon, fraud syndrome, or impostor experience) is a term initially coined in 1978 by psychologists Clance and Imes to describe describe high achieving individuals who, despite their objective accomplishments, persist in holding a belief that they are unworthy of their success and that others will eventually recognize them as a fraud . The early psychological literature on this topic (see original article) proposed that the phenomenon was prevalent among women. Since then, dozens of studies have shown that it is equally common among men and particularly troublesome among minority groups.
Professionals with impostor syndrome tend to attribute their strong performance to external factors such as luck, support from others, or extreme effort, rather than internal factors such as talent, competence, and acumen. Setbacks, on the other hand, are viewed as proof of unshakable weaknesses. Indeed, Clance described impostor syndrome as an “internal experience of intellectual phoniness in individuals who are highly successful and unable to internalize their success.” This unwarranted sense of insecurity can often result in distress, depressive feelings, anxiety, loneliness, and frustration. A recent review of over 62 studies on the topic of Impostorism showed that the prevalence rates of impostor syndrome is hard to gauge. Depending on the screening questionnaire and cutoff points used, the research showed that 9 to 82% of the participants would qualify for the label. It appears that age is negatively correlated with impostor Syndrome (i.e., it lowers as one ages). So...do you have Impostor Syndrome? Honestly, only you can answer that. If you're struggling with feelings of perfectionism, insecurity, and fear in spite of sustained academic and professional success, it is possible that you do hold beliefs that could be described as Impostorism. Many times, as hard as they might be, these feelings motivate you to keep striving and achieving, But at other times, they can stand in the way of you actually enjoying your life and the many contributions that you make to your organization. There are many ways to "treat" Impostor Syndrome. if you look in the lay media, you will find many recommendations, ranging from “own your accomplishments” to “comparing notes with peers and mentors about shared impostor feelings” and "remind yourself that you are good at what you do." I am sure those are helpful and can alleviate the suffering momentarily. However, from a CBT perspective, Impostor Syndrome is more likely a reflection of core values, intermediate beliefs and automatic thoughts that pop up in many areas of your life. Getting to those is the key to long-lasting change. You can fight Impostor Syndrome with the help of a therapist by learning to be aware of your automatic thought patterns, recognize unhelpful thinking styles, and generate alternative appraisals that help you move forward in the direction of your values and your goals.  Everyone has a sleepless night every now and then. What we do - and don't do - during the day, how we eat, what we drink, how much we exercise, our environment, our mental health, and how much stress vs. pleasurable activities we have in a typical day all influence the quality of our sleep. When insomnia hits for a night or two, it is easy to catch up. But when it becomes a chronic issue, it needs to be addressed before your health starts to suffer. One of the most effective and widely recommended treatments for insomnia is cognitive behavioral therapy (CBT).
There are two models of understanding and treating insomnia in CBT. The first approaches insomnia as the main focus of treatment. It starts by addressing behavioral modification, i.e., how long you stay in bed, and then moves on to address your beliefs about sleep. This line of treatment is often referred to as CBT-I, or cognitive-behavioral therapy for insomnia. CBT-I is shown to work better than sleeping pills, with no side effects! There are several self-help apps and websites for CBT-I. Personally, I recommend cbtforinsomnia.com, a five-week online intervention with some clinical oversight. A second model of looking at insomnia is to view it as a symptom of another, bigger emotional health problem. Often times, insomnia is a consequence of depression or anxiety. For example, patients with excessive anxiety and worry may have trouble falling asleep as their mind starts racing - worrying about tomorrow's to-dos or ruminating about past events - the minute they lay their heads on the pillow. In this case, treating the underlying disorder (anxiety) with an approach such as TEAM-CBT will lead to the insomnia resolving itself short-term. In either case, a well trained CBT therapist may be able to guide you on your path to a good night of restful sleep! I recently finished the book "Dedicated" by Pete Davis, a Harvard Law graduate who gained online notoriety thanks to a viral graduation speech in the youtube video below. Mr. Davis has expanded the concepts in his graduation speech into a bestselling book that questions how we can find commitment and purpose in a fluid society that values open choice, freedom, and individualism. It is an interesting and well-written book, focused largely on civic involvement. But as far as CBT is concerned, the sections about choice are particularly relevant. Mr. Davis makes the case for the impossibility of making "right" choices. When we call a path the "right" one, we assume that there is only one perfect future and that this one path is the absolute best way to get there. This is obviously as fallacy, as the future doesn't exist. We make it with our actions today. There are many, many choices that can conceivably lead to great places down the road. Failing to recognize that keeps us stuck in search of that one winning ticket. If we can't make the "right" choice, what we can do is make our choices right. The book quotes executive coach Ed Batista as highlighting that if we commit to the choices that we make, those choices have a much greater chance of leading us to a positive outcome. So after we make a choice, any choice, the key lever that we have to make it work well is commitment. Commitments, Mr. Davis argues, are living things. And like all living things, a commitment needs to be nurtured and nourished. When we work towards making our choices right, we are feeding that commitment and giving it a fair chance to thrive. We don't constantly revisit the choice, we don't move backwards or in circles, we don't get stuck. We commit and we move. However, like all living things, commitments can sometimes wither and fade, in spite of receiving good care. If or when that happens, it is likely time to let that commitment go, without regrets. And make a new choice. And make that choice right. In TEAM-CBT, we use the Decision Making form to help guide clients through the analytics of of a hard decision. If needed, we can process the emotions behind that choice through empathy or using a thought log. There are many therapeutic tools and interventions that can help us make careful, deliberate, well-intentioned decisions. But it is ultimately the voluntary act of committing to the direction that you choose that will make those decisions right.  Often times, thoughts that are largely accurate or even innocuous at the surface level can lead to intense sadness, anxiety or anger. For example, telling myself that “this meat tastes bad” or “I fumbled that word” or “she is not paying attention” can quickly result in a drastic mood change.
In CBT, the downward arrow technique is a way of working through these automatic thoughts to find the irrational beliefs at the base of them that are triggering the strong emotions. These beliefs may not be immediately obvious to us, so we need to ask the same questions repeatedly until we get to the bottom of it: “what does that mean about me?” and “why is it upsetting to me?”. When we get to the end of the chain, we will find a deep-seated – and mostly unhelpful – belief that explains where these intense feelings are coming from. That is called a “core belief” or “schema” and commonly builds on themes of incompetence or failure, abandonment or unlovability, and helplessness. Once these schemas are identified, we can challenge them using CBT techniques similar to the ones applied to automatic negative thoughts. Examples of Downward Arrow technique: 1) This meat tastes bad And if that were true, what would that mean about you? Why is it upsetting to you? --> I am a terrible cook And if that were true, what would that mean about you? Why is it upsetting to you? --> I am a bad mother And if that were true, what would that mean about you? Why is it upsetting to you? --> I am a complete failure 2) I fumbled that word And if that were true, what would that mean about you? Why is it upsetting to you? --> I didn’t do everything perfectly And if that were true, what would that mean about you? Why is it upsetting to you? --> People will be disappointed in me And if that were true, what would that mean about you? Why is it upsetting to you? --> I will be alone forever And if that were true, what would that mean about you? Why is it upsetting to you? --> I am unlovable 3) She is not paying attention And if that were true, what would that mean about you? Why is it upsetting to you? --> She doesn’t care about me And if that were true, what would that mean about you? Why is it upsetting to you? --> Nothing I do can make things better And if that were true, what would that mean about you? Why is it upsetting to you? --> I am helpless With good CBT techniques, you can identify your schemas and change them over time. How do we interpret the events that happen in our lives? Cognitive theory can help us get a better understanding of how that happens. The first concepts that you want to familiarize yourself with are 'assimilation' and 'accommodation.' Charlotte Nickersen wrote a very informative - and well illustrated - article with a simple overview of these concept.s
When individuals are confronted with new information that is inconsistent with preexisting schemas (i.e., stored bodies of knowledge), one of two processes occurs: assimilation or accommodation. Assimilation is the incorporation or alteration of new information to fit into existing schemas. Accommodation is the modification of existing schemas (and creation of new ones) to incorporate new events and information. Although accommodation is necessary to integrate a new experience, individuals sometimes over-accommodate when interpreting input in their environment. Over-accommodation occurs when schema changes are inaccurate and overgeneralized. Assimilation is interpreting incoming information in light of prior beliefs:
|
AuthorDr. Daniele Levy is a licensed psychologist offering CBT in-person and via Teletherapy in Menlo Park, CA. Her background uniquely combines leading edge training in behavioral sciences with deep expertise coaching and mentoring working professionals in dynamic organizations. Categories
All
|
|
This website is provided for information purposes only. No professional relationship is assumed by use of this website.
|
California License PSY 27448
Copyright © 2014 Daniele V. Levy, PhD Bay Area Cognitive Behavioral Therapy (CBT) Office: 830 Menlo Ave, Suite 200, Menlo Park CA Mailing: 405 El Camino Real #256, Menlo Park CA www.cbttherapy.com |
|
 RSS Feed
RSS Feed